WiRED’s Medical and Health Education Work in Kenya — From the Leading Medical School to Remote Villages
BY WIRED DIRECTOR GARY SELNOW, PH.D.
Preamble
Early in 2003 WiRED International launched a Medical Information Center (MIC) in the Faculty of Medicine at the University of Nairobi. U.S. Ambassador to Kenya, Johnnie Carson, gave the keynote speech during which he discussed the power of information. I’ll get to that in a minute, but first I would like to tell a brief story about an incident that took place during the ribbon-cutting ceremony.
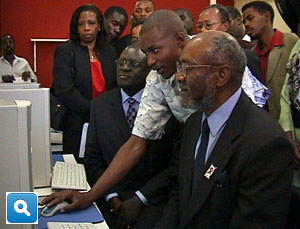
After his speech, Ambassador Carson cut the ribbon, and everyone in the crowd entered the MIC to see the computers in action. All the machines were switched on, the programs were running, and Ambassador Carson walked over to a computer and asked for a demonstration.
I signaled to WiRED’s staff member, John, a disabled young man from a particularly impoverished region of Kenya, to show the Ambassador how the computer program worked. Nervously, John leaned over next to the Ambassador, and the lesson began. A local newspaper reporter took a few photos, and, just as John was showing off a really interesting part of his lesson, the Internet crashed (Murphy’s Law is universal). John was frightened, and in a shaking voice, said this had never happened before. Ambassador Carson smiled, reached over and put his hand on John’s shoulder, then in his dulcet
tone said, “John, I wouldn’t worry about a thing, it happens to me all the time. I want you to know how much I enjoyed your wonderful demonstration. I learned a lot.” Good ambassadors know just what to say at the right time.
A few days later, the local newspaper ran a front-page photo of John teaching the Ambassador. Friends told me that when the paper came out, people in John’s community rushed the paper to John’s mother. The story goes that when she saw the photo, she fell into her chair and began to cry. Her son, who grew up in poverty and with a disability, had almost no expectation of advancement. Few people from these surroundings got anywhere; most lived a hardscrabble life; some did drugs and alcohol, and most died young. Yet here on the front page of the newspaper was her son teaching the Ambassador of the United States of America. For John’s mother and the community, that was a remarkable day.
The Medical Information Center
Our work in Kenya during the past two decades has taken us from the country’s leading medical school in Nairobi to the ordinary villages in backwaters of this extraordinary country. WiRED’s health education programs have evolved since our early days, and, with new features, continue to operate today in Nairobi and in northwestern Kenya. Moreover, our health education work has expanded through the labor of young people we taught many years ago, who now have set up their own health organizations and programs. That has been a gratifying development.
In this chapter on WiRED’s history, I would like to offer a few stories about our early work in the largest medical school in the country and in the small towns where our health education programs reach average Kenyans every day. I will conclude with an afterthought about lessons we learned in Kenya that apply to populations around the world.
The First Medical Information Center in Kenya
Early in 2003, Pauline Karani, WiRED’s program coordinator in Kenya, and I met with Professor Dominic Makawiti, Dean of the Faculty of Medicine at the University of Nairobi. The school’s library had few journals and books, and a lack of funding meant there would be little improvement any time soon. Computers had not yet been introduced to the library or to the medical school, so electronic medical resources that were becoming available elsewhere in the world were beyond the reach of Kenya’s leading medical school.
Pauline and I described for Dean Makawiti WiRED’s Medical Information Centers (MICs), which, at the time were operating in the Balkans and soon would be in Iraq. We asked if he would accept our offer to supply the school with the necessary equipment and software to run WiRED’s programs. We said we would network 10 computers, connect them to the Internet and provide an extensive collection of CD-based medical courses. Computer technology would instantly deliver a trove of material beyond anything the school could ever hope to provide in print form. 1
Professor Makawiti, who today is a member of the prestigious Kenya National Academy of Sciences, was well aware of the information revolution taking place elsewhere, and he immediately accepted our offer for the MIC. With support from the U.S. National Institutes of Health and WiRED’s individual donors, we set up the center, supplied our CD training library and got the system online. It was the first such computer facility established at a medical school in Kenya and perhaps in East Africa.
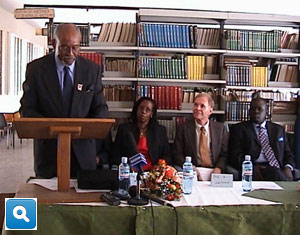
The launch
We usually try to launch a new MIC with a small celebration and a few speeches. The grand opening this time was especially grand because the U.S. Ambassador to Kenya, Johnnie Carson, agreed to deliver the keynote address. Ambassador Carson, a well-known and well-respected figure throughout Africa, believed strongly in education to advance national progress and personal empowerment. Specifically, he recognized the importance of education in furthering Kenya’s role in the world. He saw WiRED’s MIC as a valuable instrument in medical education when he said:
As a result of this information explosion, it is extremely important for medical students and their faculty to have access to the most up-to-date research findings and new information in their fields. This computer center, with its CD library and Internet access, will enable the future doctors, nurses and dentists of Kenya to be as well-informed as their counterparts in the rest of the world.
Ambassador Carson also recognized that the MICs were a source power for Kenyans, and he called it knowledge and information power:
I want to say something about this center in relation to our two nations. First, it seems that the image of the U.S. often focuses on our military and economic power. This center, and the WiRED program in general, is a demonstration of another type of power — the power of knowledge and information. I'm proud that the U.S. is a world leader in the area of information and knowledge power — and I'm delighted that WiRED is helping in the effort to share this with the people of Kenya. In the long run, this form of empowerment, the sharing of the power of information, is more important than any other form of power in the 21st century.
Ambassador Carson cut the ribbon to the new center, and the library, typically short of visitors, was filled with students and professors using the new computers for academic research. We had seen similar enthusiasm for a new MIC among medical professionals in other countries. Here in Nairobi, the CD-ROMS offered expert training programs, and the budding Internet provided the same real-time information that was available to the best medical schools and hospitals in the world.
Since we opened the Nairobi MIC nearly 15 years ago, advances in information technology have accelerated, and new tools and resources have become available. The heavily-used computers were updated, repaired and eventually replaced. In 2003, the first computers provided information access at a critical time and launched medical students into an information age that now is central to the study and the practice of medicine around the world. WiRED’s volunteers are happy to have had the opportunity to be part of this process in Kenya.
Stories from the field
Two important early decisions
Through the mid-2000s, WiRED operated 21 Community Health Information Centers (CHICs) in Kenya. The CHICs were located in public places — usually in shops, non-profit facilities and community buildings — where people could walk in and use the equipment for free health education. Initially, our plans were to focus on HIV/AIDS, which was ravaging populations across Africa. The U.S. National Institutes of Health provided WiRED with a grant to test the concept of using computers to teach people about the prevention, diagnosis and treatment of HIV/AIDS. We purchased the equipment, acquired or developed the software and set up the CHICs. To operate them, we hired and trained local people in computer technology and in the medical details of HIV/AIDS.
During the planning stage, well before we set up our first center, we learned that few people would want to be seen entering a facility specializing in HIV/AIDS. To do so would tag them with the AIDS label; they would be seen as infected and as persons to avoid. So, calling these facilities HIV/AIDS Education Centers would doom them from the start; no one would show up.
Accordingly, we made two critical decisions. First, we expanded the project scope to teach people about a wider range of illnesses. We included infectious diseases, such as malaria, cholera, tuberculosis and influenza; and chronic, non-infectious diseases, such as hypertension, diabetes, stroke and cancer, all of which were endemic to Kenya. Of course, we included an extensive collection of training material on HIV/AIDS, but blended it into the mix of other topics.
Our second decision, accordingly, was to give the centers a name that reflected the broader range of topics. Rather than HIV/AIDS Centers, we called them Community Health Information Centers, which quickly became known everywhere as CHICs. Thus, the name and the expanded health curriculum avoided the stigma and broadened the usefulness of these centers, allowing people to learn about HIV/AIDS but also about many other life-threatening illnesses that Kenyans confront every day.
Very soon we discovered a pattern: People would come to the centers, request training modules on say malaria or hypertension, but quite often, in a hushed tone, ask the CHIC staffer for information on that other disease, what was it called now . . . oh, yeah, HIV/AIDS. Expanding the library of modules to include other topics made it easy for people to be seen in the centers and also to learn about HIV/AIDS.
The traditional healers
In Kenya, as in many countries throughout Africa, illnesses are treated by physicians who were educated in medical schools and who practice science-based medicine, and also by traditional healers who were trained by elders and who practice herbalism, homeopathy and other forms of alternative medicine. While both treatment approaches are available throughout Africa, physicians and science-driven medicine are more common in urban areas, while healers and traditional medicine are more common in rural areas.
Although some people might discount the legitimacy and effectiveness of the alternative medicine practiced by traditional healers, people in towns and villages where traditional medicine dominates place great credence in these practices and display considerable reverence for the skills and judgment of the healers.
Since we put a number of our CHICs in places where traditional medicine was practiced, we wanted to avoid a potential conflict between our centers’ science-based information and the population’s traditional medicine. In particular, we were concerned about the reactions of traditional healers. After all, we were outsiders coming into their villages. Although we hired local staff for the centers, some people might see us as intruders, trampling on local customs and challenging the revered traditional healers. Would the healers themselves see us as treading on their turf and meddling in their business? I thought that would be a reasonable and rational reaction. Moreover, we wondered whether local people would avoid the CHICs, or worse, run us out of town? We just didn’t know.
Based on the wise counsel of Pauline Karani, our Kenyan coordinator, and other staff members, we always partnered with local groups when we set up a facility and never opened a CHIC on our own. This reflected our belief that each center needed a strong local connection, and we hoped this might help avoid potential problems with traditional healers. If no one in a community wanted to work with us, we avoided that village or town.
The next thing we did was hold a frank and open meeting with our partners, our Kenyan staff and local leaders, including traditional healers. We explained why we were there, what we were planning to do, and how it would help the people of the village. We demonstrated the computers and the health training software and invited the healers and local leaders to try the programs themselves.
We also had forthright conversations about HIV/AIDS, clearly a leading but rarely discussed health concern. In most places where we held sessions, we learned that the healers had encountered the full force of the AIDS outbreak in their populations. We also saw that they just didn’t understand the illness. Their experience in human health included nothing like this disease that struck entire villages, generally sparing young children and old people but wiping out so many people in their middle years. Nothing they offered cured the illness, no remedy eased the symptoms or prevented ultimate death. Some believed the disease was caused by witchcraft; some suspected that the victims had character deficiencies. The condition of the wasting victims cast a dark shadow on anyone who contracted AIDS. The healers were as perplexed by this illness as physicians had been only a few years earlier.
We made traditional healers an offer: We would provide them with a special training program. They could review all the material we would make available to the community. They could spend as much time as they wished with the programs and with our staff; they could question the information and tell us if they disagreed with anything they saw. They always accepted the offer.
WiRED’s local Kenyan staff held classes, walked the healers through the details of HIV/AIDS, explained that it was a virus, described how a virus takes over a cell and how diseased cells ultimately bring down the host. They explained that there was no cure or treatment (anti-retro viral drugs were not yet available), but that the illness could be prevented by avoiding unprotected sex with an infected person. That explained the age patterns and disease progression the healers were seeing. In most cases, they understood and accepted the scientific account of the disease.
We were encouraged by the healers’ responses. We offered them two- or three-hour blocks of time, reserving the CHICs just for them. They could use the computers, and our trainers would work with them on HIV/AIDS and other illnesses that plagued this part of Africa. Our aim was to discuss these conditions and explore preventive measures. We described our treatments with science-based medicine and did not promote our remedies as the only solutions. The discussions went both ways. The healers explained to our staff their approaches to healing and to the medicines they formulated from local plants. In most regions, the CHIC staff and the traditional healers developed an amicable relationship which resulted in positive outcomes.
The healers also could use the CHIC facilities for meetings. In Butula, a small town in northwestern Kenya, the meetings led to the formation of an organization of traditional healers, which they registered with the Kenyan government. Such a step was unprecedented, and I could see that the healers took considerable pride in this accomplishment. The CHIC provided the programs and the place that helped lead to this outcome.
The traditional healers became strong promoters of the CHICs, especially when they encountered people with AIDS. When they saw signs of AIDS, they told the patients to visit a center to learn about the illness and to ask about testing. While WiRED did not have a testing facility, we became strong advocates of VCTs — Voluntary Counselling and Testing Centers, which were available throughout the country. VCTs had on-premises testing tools and on-hand counselors who could work with people who tested positive. WiRED referred people to the VCT counselors, and they in turn encouraged HIV-positive people to visit the CHIC to learn about their illness, learn how to improve their health and learn how to avoid transmitting the illness to others.
We went into this project with some hesitation about the likelihood that we could overcome a natural resistance to outsiders’ arriving with computers and talking about science-based medicine. Despite our uncertainty, we were happy to find that almost every case resulted in a positive and successful outcome.
Afterthought
The project ran for three years, and the successful results of the concept were compelling. The centers were popular in local communities, and the training programs effectively taught people about better health and health practices. Funding from our development grant ended, but WiRED continued to support a reduced number of centers with small donations from individuals and organizations. Today, the program operates in Kenya with new equipment and educational material and new models of instruction. We’ve added community outreach programs for schools, churches and community groups, going directly to the people with laptops and projectors for group sessions and not requiring them to come to a CHIC (although the doors are still open).
We’ve added a certificate program that allows people to study a collection of modules, successfully pass exams and earn certificates reflecting the number of modules they completed: a bronze certificate for five, a silver certificate for 20, all the way up to a platinum certificate for 50. At our graduation last fall, 85 people earned certificates.
We also have augmented programs for community health workers and medical professionals who often have few options for continuing medical education. The CHICs and outreach programs offer material to medical practitioners that allow them to stay current and to learn new skills.
We use the lessons we learned in Kenya in our programs around the world. The profiles of illnesses may vary, but the same health conditions that affect Kenyans affect everyone. Moreover, people everywhere have the same need for information to help themselves and their families prevent diseases and treat diseases when they strike. This is no surprise, but in our education work we are reminded every day of our shared frailties and vulnerabilities, concerns and hopes for good health.

This is the fifth story in a series about WiRED International. How it evolved; how it went from providing computers and Internet connections for towns and villages in underserved regions to focusing on medical and health education using computer technology. How it expanded its work throughout the Balkans to Africa, Central and South America to the Middle East and Eurasia. How WiRED’s training programs, carried by the Internet, have now become global resources, used by hospitals and clinics, schools, other non-governmental organizations and universities.
An element of WiRED’s operation that repeats in every story is that all of WiRED’s programs are run mainly by volunteers who have made it possible for WiRED to provide medical and health training programs cost-free to everyone. WiRED’s administration is volunteer, we have a volunteer board, and our writers and editors are volunteers. A small paid staff builds and shepherds the training modules through the production process, but even their work is augmented by that of volunteers. I’m proud of the people in the United States and abroad who donate their time and lend their talents to this organization’s efforts to provide people in low resource regions with some of the finest public-access, health training material available anywhere.
1 HINARI description:
Among the medical education material coming online in those early days was the remarkable HINARI program, organized by the World Health Organization (WHO), that consolidated material from a host of leading medical journals, books and research monographs. HINARI material was free to the poorest countries, such as Kenya, and so the latest published medical research was instantly available, without cost. WiRED tips its hat to WHO for negotiating these resources with publishers and for making them available online to medical professionals and students in low-resources regions around the world.
This is a description of the current HINARI program:
Low- and middle-income countries can gain access to one of the world's largest collections of biomedical and health literature. Up to 14,000 journals (in 30 different languages), up to 53,000 e-books and up to 105 other information resources are now available to health institutions in more than 115 countries, areas and territories benefiting many thousands of health workers and researchers, and, in turn, contributing to the improvement of world health.
^ Back to the Top